This will blow your mind....
52 year old male presented to the emergency department with chest pain. A CT angiogram of the aorta was ordered, which showed a mildly dilated ascending aorta (about 4.6 cm at sinuses of Valsalva), without acute aortic syndrome. There was very poor enhancement of the pulmonary artery (<100 HU).
On lung windows, a ground glass opacity was seen in right lower lobe. with a central dense infiltrate.
On spectral analysis, clear defect seen in right lower lobe pulmonary artery at 40 keV mono-energy image, consistent with pulmonary embolus. The lower keV images enhance vascular contrast, and attenuation in the pulmonary vascular system is >200 HU.
Pulmonary embolism was confirmed with a dedicated CT PE exam.
So far this is fairly routine stuff. I then started looking at lung perfusion. On the CTA of the aorta, the central dense infiltrate in the right lower lobe shows no perfusion, but surrounding ground glass opacity shows increase iodine uptake. On CT PE study, the entire area (ground glass opacity and central infiltrate) show decreased perfusion.
I believe this is the first ever sighting of an ischemic penumbra in the lung, with increased transit time, and retention of iodine on the aorta CTA (where acquisition is later) serving as indicator of increased blood volume. The central core of infarction shows decreased iodine uptake on both the early and delayed scan.
I wonder if this information can be used for risk stratification, and assessing treatment response. Using spectral to better understand physiology sure blows my mind...
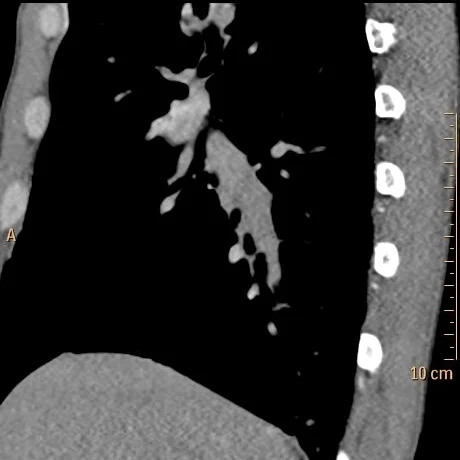
Conventional CT (oblique sagittal) shows normal appearing right lower lobe pulmonary artery

Same slice as above, 40 keV mono-energy image sgows right lower lobe pulmonary artery filling defect consistent with pulmonary embolism

CT chest PE protocol confirms pulmonary embolism in right lower lobe

Oblique sagittal image lung windows shows infiltrate in the costophrenic angle with surrounding ground-glass opacity
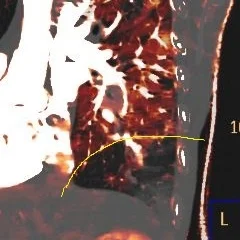
Iodine overlay image on CT PE study shows large perfusion defect in right lower lobe (outlined in yellow)

Iodine overlay image on CT Aorta shows the central core of decreased perfusion (outlined in yellow), and a peripheral zone of increased perfusion (outlined in blue). I beleive this is the penumbra.