Pulmonary septic emboli
27 yo M, h/o IV drug use, presented with chest pain. CT with contrast performed according to the PE protocol shows a 2.2 cm nodule in the peripheral right upper lobe, with a subtle central cavitation.
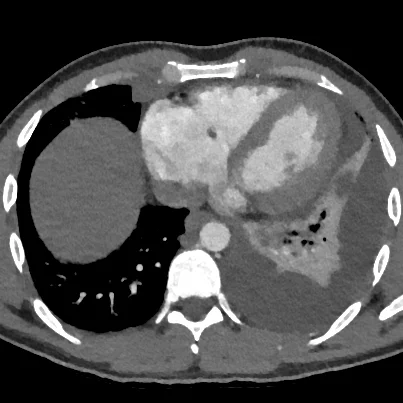
On spectral analysis, the nodule has markedly decreased iodine uptake. This case is somewhat unusual in that patient aslo has a obvious pulmonary artery embolus in the right lower lobe.
Careful analysis shows a small filling defect adjacent to the tricuspid valve, and a dilated right atrium. Tricuspid endocarditis confirmed on echocardiography.
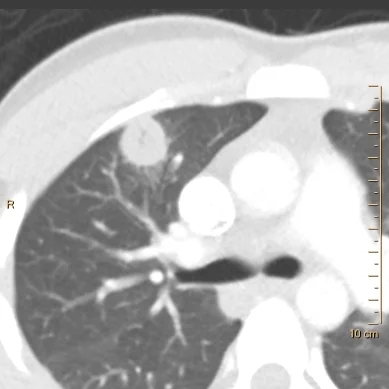
Conventional CT shows right upper lobe nodule with subtle cavitation

Iodine map shows markedly decreased iodine uptake in the nodule

Iodine uptake in nodule is about 0.13 mg/mL (vs 1.58 mg/mL in normal lung)

Large embolus in right lower lobe
Note subtle vegetation adjacent to the tricuspid valve
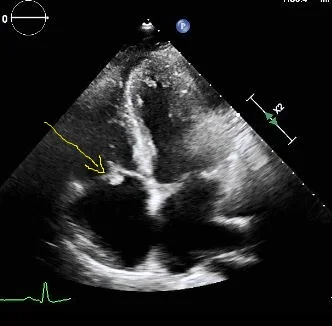
Image from transthoracic echocardiogram confirms vegetation on tricuspid valve (yellow arrow)