Coital cyst rupture
38 year old female who had been “engaging in intercourse with her significant other for >2 hours” when she had sudden onset of pelvic pain during vaginal intercourse. She waited for a bit, thinking it was a pulled muscle, but the pain intensified and she came to the ED. Previous h/o hysterectomy.
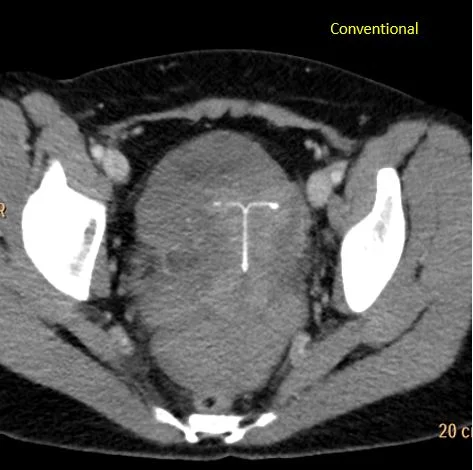
CT scan obtained in the ED shows a complex right adnexal mass, about 60 HU. Turn on spectral CT, and you see it is made of non-enhancing clot, hyperdense on virtual non-contrast and without iodine uptake, inside the thin, enhancing lining of a cyst. The clot has a spectral curve that is flat, consistent with absent perfusion.
Pain improved with medication. She was observed in the hospital, and discharged on the next day.
CASE 2
30 year old female with acute onset pain that radiates to her shoulders. Abdomen tender on exam, UPT negative. CT scan obtained, shows large hemoperitoneum with dense clot in the pelvis. Hard to separate clot from the uterus.
On Spectral analysis, easy to separate clot from the uterus. There is also a 1.9 x 1.2 cm right adnexal cyst. Ultrasound shows cyst is likely an involuting corpus luteum.
On further questioning, pain started shortly after intercourse. Patient remained uncomfortable, and was eventually taken to the OR, where a large hemoperitoneum was evacuated, and a right adnexal cyst with wall defect was confirmed.
Both these cases show something I see quite often. Intuitively, it makes sense that adnexal cysts can rupture during intercourse, and a hemoperitoneum can be very painful, of course. It is kind of odd that I can only find the occasional case report, although this phenomenon has been described in the lay press (careful: somewhat explicit link which interestingly has the WRONG CT image as well). I wonder if it has to do with the “sensitive” nature of the topic.
These patients often get CT scans, and using spectral CT, we can differentiate between clot and adnexal structures/uterus very well, and can often see the cyst that has bled. Of course, you need to make sure the UPT is negative, as a ruptured ectopic can look exactly the same.
In the first patient, there was only a small hemoperitoneum, so she was managed conservatively. When there is a large amount of blood present, as in case 2, patients will often end up going to the OR. In any case, they will usually do very well.
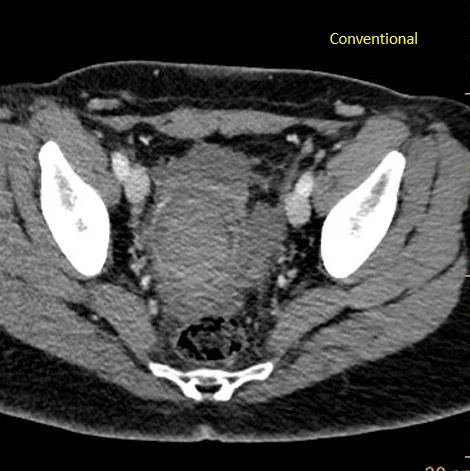
Patient 1: Conventional CT shows right adnexal "mass”.
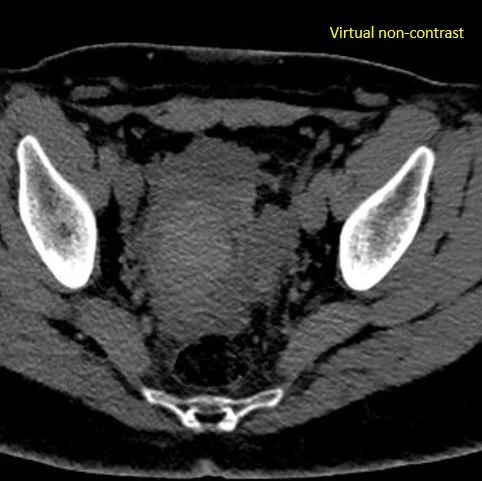
Virtual non-contrast: Dense clot in the mass.

Iodine map: No uptake in the mass. Notice the thin enhancing margin. This is a blood clot inside a cyst.
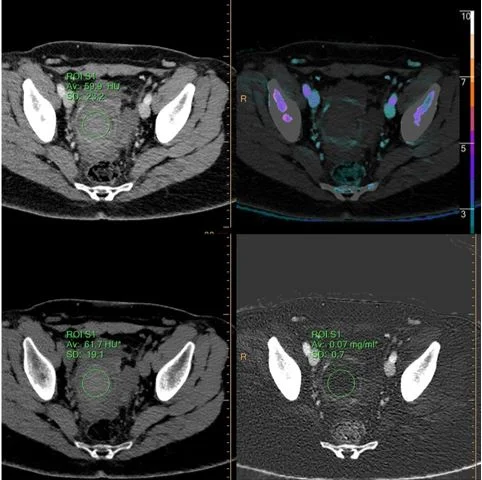
ROI on the clot shows no enhancement, and no iodine uptake.
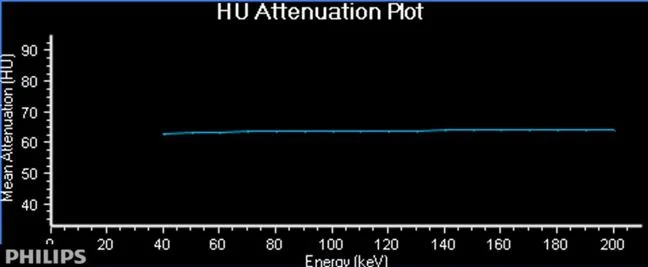
Flat spectral curve confirms lack of perfusion.
Ultrasound shows absent flow in the clot.
CASE 2: Coronal CT shows large hemoperitoneum.
Conventional CT: Just a big mess in the pelvis.

Iodine map: See perfusion to the uterus, and absent perfusion posterior, c/w clot.

VNC: Large clot posterior to the uterus is hyperdense.
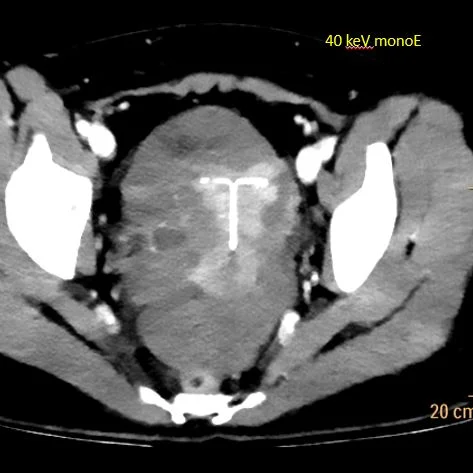
40 keV monoenergy image shows small right adnexal cyst.
Ultrasound confirms right adnexal ruptured corpus luteum.