The case of the two infarcts
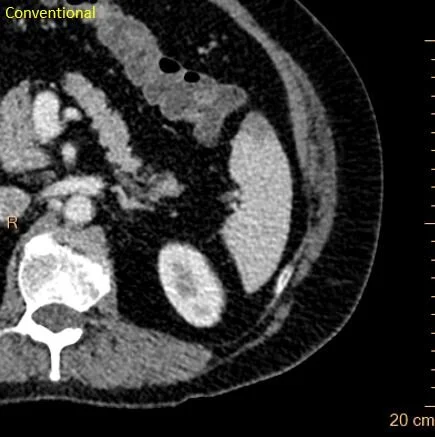
55 yo F with long-standing Crohn disease presents with abdominal pain. CT scan shows distal small bowel obstruction, with mucosal hyperenhancement, consistent with a Crohn related stricture. There are wedge shaped hypodensities in the right kidney with absent iodine uptake, consistent with infarcts.
Echo was negative. Patient managed symptomatically, and discharged after a few days. Two weeks later, patient returns with abdominal pain. Again, a CT is performed, and shows a very subtle hypodensity in the anterior spleen with absent iodine uptake, consistent with splenic infarct.
Now, with 2 separate organ infarcts, you have to really worry about a central source of embolism. Remember that Echo does not rule out all the potential sources of clot, and a CT is a good idea.
CT shows linear filling defect in ascending aorta. We worry this is a dissection, but looks odd. So we do a gated CT, which shows mobile wall-adherent thrombus in the ascending aorta. The video is heart-stopping, and on my twitter feed (@CtSpectral).
Patient decided to pursue conservative management with anti-coagulation. Clot resolved 3 months later, no complications.
Moral of the story: Look for organ infarcts with spectral CT, and when you see them, chase a source, almost always you will find one. CT will compliment a negative echo.

Oblique axial iodine overlay shows inflamed loop of terminal ileum (red arrow). Note upstream dilatation.

Hypodensity right kidney lower pole. Could be pyelonephritis or infarct.
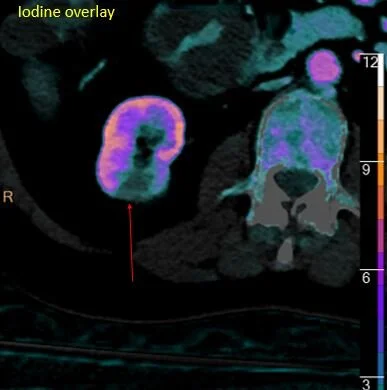
Absent iodine uptake. Still could be pyelonephritis or infarct.
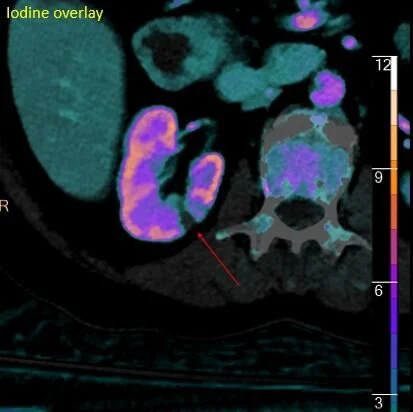
Here is another hypodensity. UA was clean. So these are most likely infarcts.
CT 2 weeks later: Do you see the spleen hypodensity?
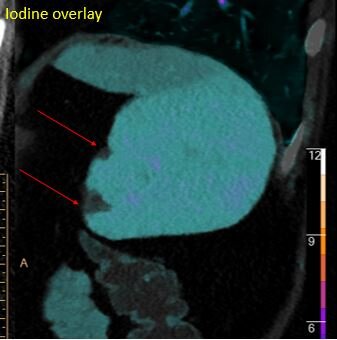
Iodine overlay shows there are actually 2 infarcts present (red arrows).
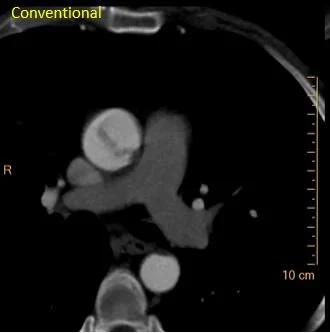
Odd linear filling defect in aorta
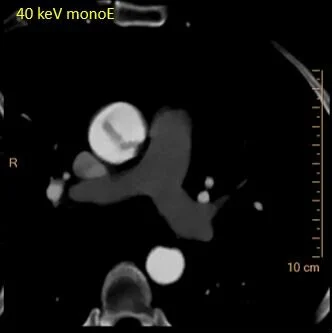
The filling defect is confirmed on 40 keV image.
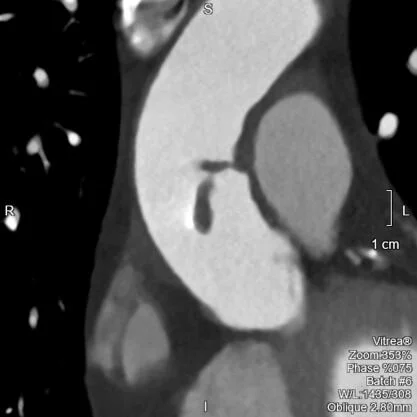
Gated CTA shows filling defect is mobile. Video on my twitter feed (@CtSpectral).