Filling defects and iodine maps
Two separate cases presented.
60 year old male with profound psychiatric impairment presents with chest pain. A CT scan was obtained, with thickening and a "filling defect" in the bronchus intermedius. These are usually debris, but as you turn on spectral, notice the clear iodine uptake in the filling defect. Subsequent CT shows increased size, and intense uptake was seen on PET scan. Bronchoscopic biopsy confirmed squamous cell carcinoma.
58 year old male presents with chest pain and shortness of breath. CXR shows left upper lobe atelectasis. CT scan showed left hilar mass, and "filling defects" in the left lower lobe pulmonary arteries, consistent with pulmonary emboli. Turn on spectral, and there is clear iodine uptake in the pulmonary emboli. There is intense uptake of FDG on follow-up PET scan, and this is therefore tumor embolism.
These cases illustrate why it is important to add spectral reconstructions to every case: they add value! It will significantly increase your confidence in making diagnoses and will show you things you would not expect to see.
Most rads would be suspicious of the bronchial lesion, but spectral can make you certain there is a tumor there. And I doubt many of us would be able to call the tumor emboli: remember that cancer patients have a very high incidence of bland pulmonary emboli.

Case 1: Conventional CT with thickening of bronchus intermedius and a filling defect (red arrow).
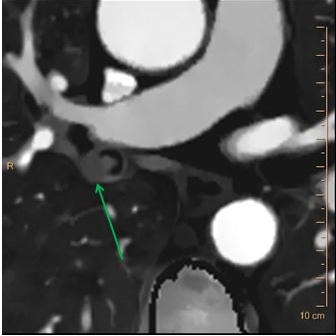
Case 1: iodine map with clear uptake in lesion.

Virtual bronchosopy shows lesion now growing in the right mainstem bronchus (yellow arrow, remember this image is oriented like an optical bronchoscopy).
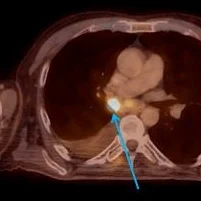
Case 1: PET scan with intense uptake in the bronchial lesion.

Case 1: Optical bronchoscopy confirms mass, Biopsy was also obtained.

Case 2: CXR with classic left upper lobe atelectasis. This one is for residents!

Case 2: lateral view confirms LUL atelectasis. Needs a CT right away!

Case 2: Filling defects in left lower lobe pulmonary artery branches (red arrow).

Case 2: Filling defect with clear iodine uptake (red arrow).
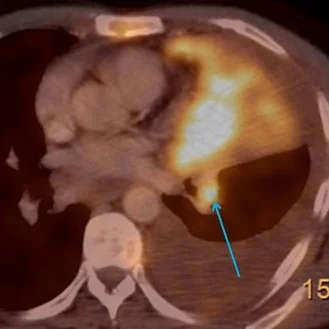
Case 2: Intense uptake on PET scan (blue arrow)