Imaging 3.0: How spectral CT can help
83 y.o. male with ischemic cardiomyopathy (EF 38%), CAD, chronic kidney disease (stage 3), aortic stenosis s/p TAVR admitted for abdominal pain, nausea and vomiting. Estimated GFR 43 mL/min/1.73 m2 BSA. CT angiogram of the abdomen with reduced contrast load, requested after radiologist and physician consultation.
Scan performed with 60 mL injection at 4 mL/sec, using 50% contrast (30 mL contrast load). Mesenteric vasculature is patent. Diffusely dilated loops of small bowel, with a focal cluster of hyperdense loops with engorged mesentery in the right upper quadrant in a radial configuration. A closed loop obstruction was called, and patient taken to the OR urgently.
Is the hyperdense closed loop inflamed, or is it something else? On spectral analysis, virtual non-contrast shows bowel wall in the closed loop remains hyperdense, suggestive of hemorrhage. There is no iodine uptake in the closed loop. On surgery, a 20 cm closed loop "black, purple, and necrotic appearing" was found. Bowel resection and primary anastomosis was performed. Path confirms a completely necrotic loop with transmural hemorrhage
Spectral CT can help with "imaging 3.0". The exam was done is a safer fashion, after radiologist consultation, using a lowed dose of iodinated contrast. Virtual non-contrast eliminates the need for a true non-contrast phase, reducing radiation dose (admittedly, not of primary importance in a 83 year old, but the principle stands). The combination of virtual non-contrast and iodine map (even with reduced contrast load) enables a prompt diagnosis of closed loop obstruction with hemorrhagic necrosis (truly an actionable report), expediting surgery and correlating beautifully with pathology.
Patient did fine post-op, GFR at discharge was 66 mL/min/1.73 m2 BSA.

Conventional CT, oblique coronal plane: Closed loop in right abdomen (note the radial arrangement)

MIP image (50 keV mono-energy reconstruction) shows excellent opacification of the aorta on CTA with 30 mL contrast

Sagittal MIP image (50 keV) shows patent celiac artery and SMA

Conventional axial image with closed loop in right lower quadrant

Virtual non-contrast: wall of closed loop remains hyperdense consistent with hemorrhage

Iodine density image: closed loop in right lower quadrant without perfusion. Note loops in left lower quadrant with intact perfusion. The iodine map has poor signal becuase of the low contrast dose technique used.

Iodine overlay image confirms ischemic loop

Gross path (courtesy of Dr. Cameron, HCMC): resected loop is "black and blue"
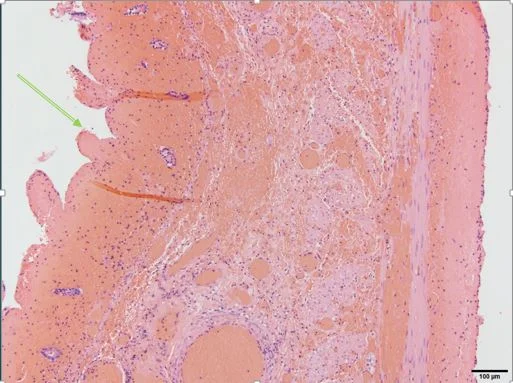
Histopath (courtesy of Dr. Cameron, HCMC): Transmural hemorrhage (all that red stuff) from the mucosal side (green arrow) to the serosa. The loop is completely necrotic.
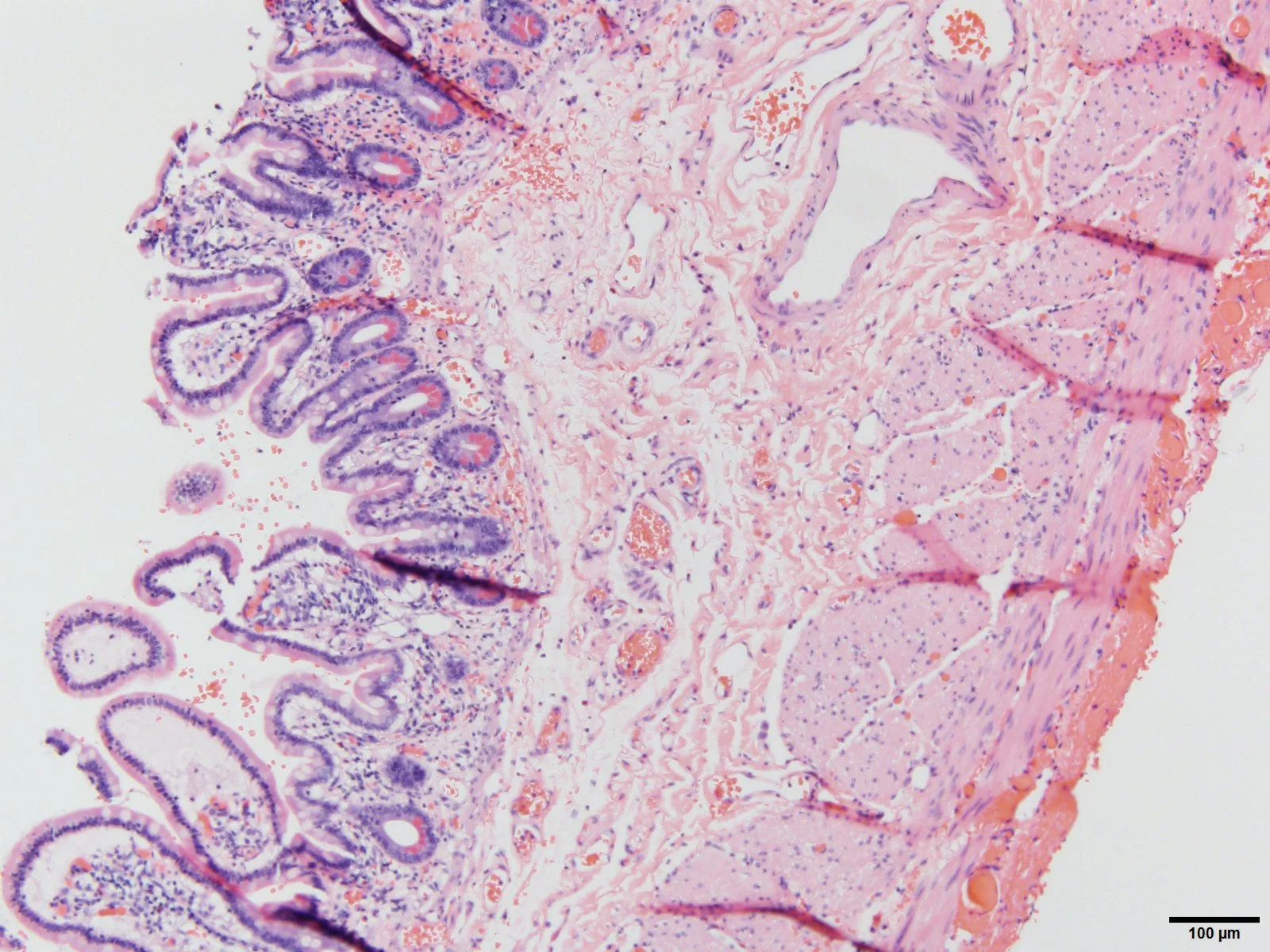
Histopath (courtesy of Dr. Cameron, HCMC): Viable bowel at the margin. Note the healthy mucosa, and a small amount of serosal hemorrhage