Hypoxemia in Osler-Weber-Rendu
66 year old female with long-standing polycythemia, found to be hypoxemic on exam (O2 sat 93% on room air). Chest X-ray shows persistent right lung "infiltrates", so a chest CT was performed. There is a history of AV malformations in the brain and colon.
Routine chest CT is straightforward: a large complex AV malformation is seen in the right lower lobe. Feeding artery is 8 mm. There are probable additional multiple tiny AVM's in the lungs. Patient most likely has Osler-Weber-Rendu or hereditary hemorrhagic telangiectasia.
Spectral CT shows shunting of blood from healthy alveoli around the AVM into the low pressure pulmonary venous circulation as a paucity of iodine in the right lower lobe anteriorly. This illustrates the part of the physiology involved in the disease.

Volume rendered image shows large right lower lobe pulmonary AVM. Note supplying artery (blue arrow) and draining vein (red arrow).
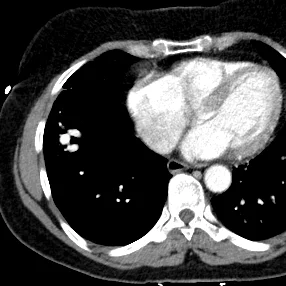
Pulmonary AVM seen on axial image

Iodine map shows perfusion deficit seen around the AVM

Iodine map in the coronal plane nicely illustrates the pulmonary AVM and adjacent perfusion defect. This is because of blood (and iodine) shunting into the low pressure system, and results clinically in hypoxemia, that then sets off compensatory mechanisms resulting in polycythemia.

Iodine overlay image illustrates same finding.