Do we really need a true non-contrast scan for aortic imaging?
67 yo M presents with chest pain. Prior history of CABG.
A routine CT angiogram of the aorta was performed. A Stanford type A dissection is seen, with a partially thrombosed false lumen. Turn on spectral, and the thrombosed false lumen is seen as a high density crescent about the ascending aorta on the virtual non-contrast.
Lower down in the abdominal aorta, we see plaque at the level of the inferior mesenteric artery, confirmed by low density on virtual non-contrast.
The ascending aortic dissection was surgically repaired.
We do not do a true non-contrast acquisition for imaging the aorta. It does not add anything but radiation.

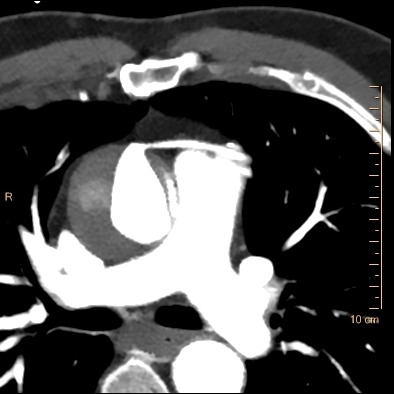
Conventional CT through ascending aorta. Note dissection flap on the left side of the aorta, and the saphenous venous graft anteriorly. The low-density crescent on the right side of the aorta is why we do non-contrast scans: it can be hard to tell intramural hematoma/thrombosed lumen versus plaque once you have given contrast

Virtual non-contrast image nicely depicts increased density to the right of the ascending aorta, in this case, a thrombosed false lumen
40 keV mono-energy image nicely depicts small amount of flow centrally

Conventional CT just above aortic valve. Note the type A dissection, with some contrast in the false lumen.

Mural irregularity at the level of the IMA in the abdominal aorta, this could be plaque or intramural hematoma.
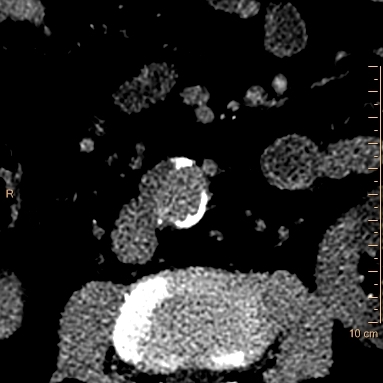
Low density on virtual non-contrast confirms plaque. This does not require intervention.