The hole and the hot rim
Elderly male presents to the ER with right upper quadrant pain for the last several days. White count is elevated. Point of care ultrasound shows no gallstones. A CT scan is performed. Conventional images show no calcified gallstones, but the gallbladder wall is thick, and there is fat stranding next to the gallbladder wall, consistent with acute cholecystitis.
So now what? The gallbladder needs to come out, but how urgent does surgery need to be?
Look at spectral CT images: On the 40 keV image and iodine map, there is a focal defect in the gallbladder wall enhancement. This is consistent with focal necrosis. No negative gallstones are visualized on spectral imaging (this is one of my favorite applications of spectral CT).
Surgery confirmed necrotic cholecystitis, with gross purulence. Path report mentions a 1 cm hole in the gallbladder. Patient recovered uneventfully postop, a delay in diagnosis could have led to a very different outcome.
Interestingly, this recent paper compared US vs CT for acute cholecystitis (very few direct comparisons available) and found that CT was much better test. I believe they are probably right, US is vastly overrated for this application, in my experience.
Spectral CT goes above and beyond: by depicting necrosis, patients can be appropriately selected for emergent surgery.
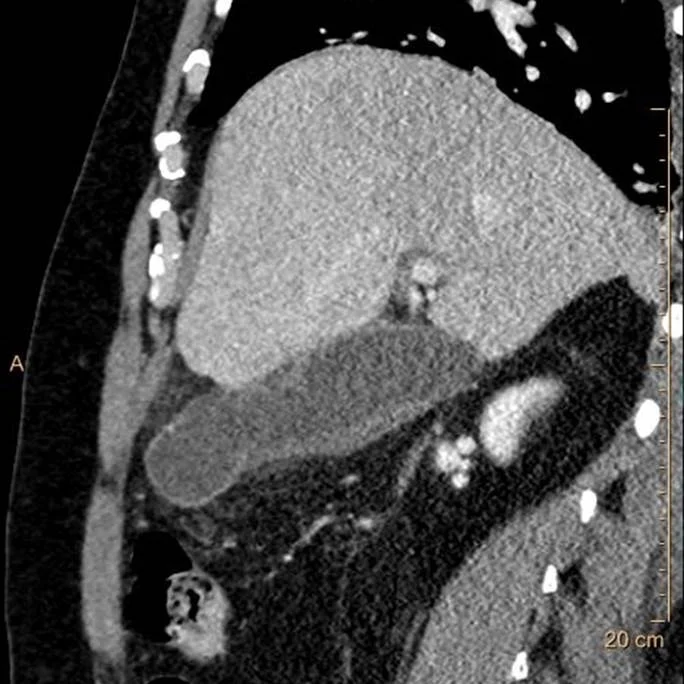
Conventional CT, sagittal image. Thick gallbladder wall with adjacent fat stranding, consistent with acute cholecystitis.
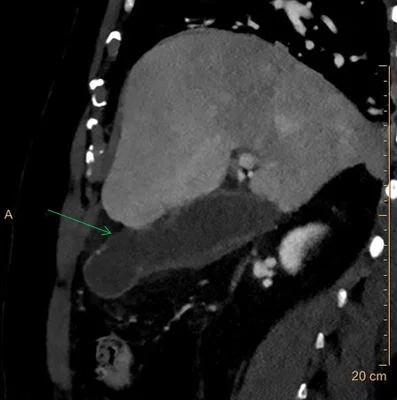
40 keV image: Clear disruption in wall enhancement (green arrow). No negative gallstones are seen.
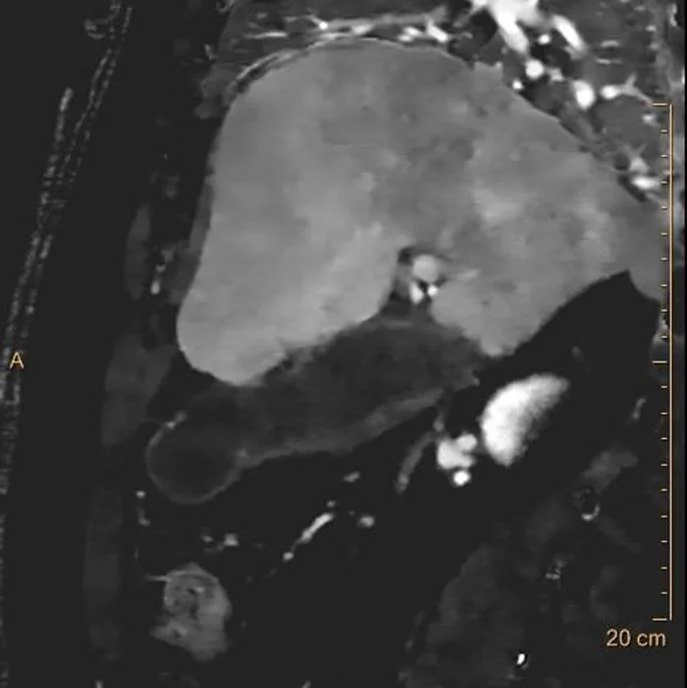
Iodine map also shows the same “hole”. Discontinuous enhancement is a very good sign of necrosis or perforation.
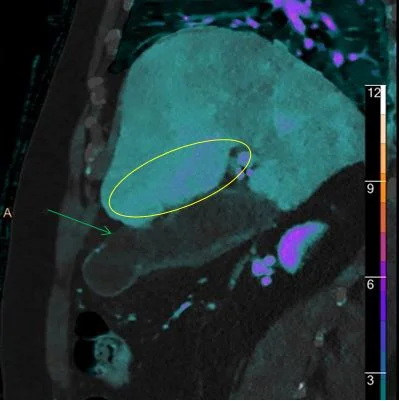
Iodine overlay shows the “hole” very well (green arrow). For nuclear medicine aficionados, see the enhancement in the liver adjacent to the GB fossa (yellow oval), equivalent to the “hot rim sign” so well known from HIDA scans.