Let us solve this one...
44 year old female with history of gastritis presents with abdominal and chest pain. Pain is located diffusely over upper quadrants and radiates up to chest and back, described as crushing, associated with difficulty breathing. Patient also endorses having pain in upper extremities, described as numbness/tingling worsen her left arm associated with weakness.
EKG was not significantly changed from baseline. Troponin came back positive. A CT angiogram of the chest was performed which was negative for aortic pathology. Echo showed no focal wall motion abnormality.
Patient taken to cath lab: mild plaque, no angiographically significant obstructive coronary artery disease found.
So now what?
Cardiac MRI performed a few days later: Small (about 1.2 cm) transmural infarct in the inferior wall.
Now let us go back to the CT scan. The conventional images through the heart are underwhelming. Turn on spectral CT, and there is an obvious perfusion defect in the inferior wall, corresponds exactly with the focus of delayed enhancement on MRI!
As we do more spectral CT imaging, we will see more mysteries like this solved, or not mystifying in the first place. This was likely a small thrombotic coronary occlusion that resolved by the time of the catheter angiogram, with scar well depicted on subsequent cardiac MR. Patient was treated as a NSTEMI.
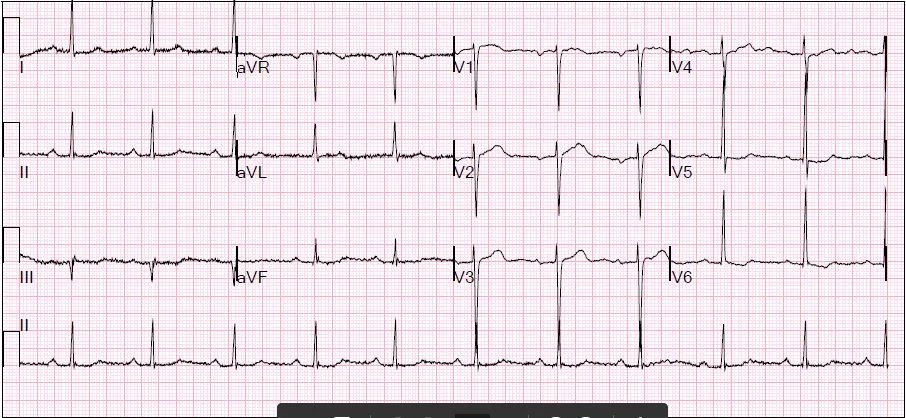
EKG is inconclusive
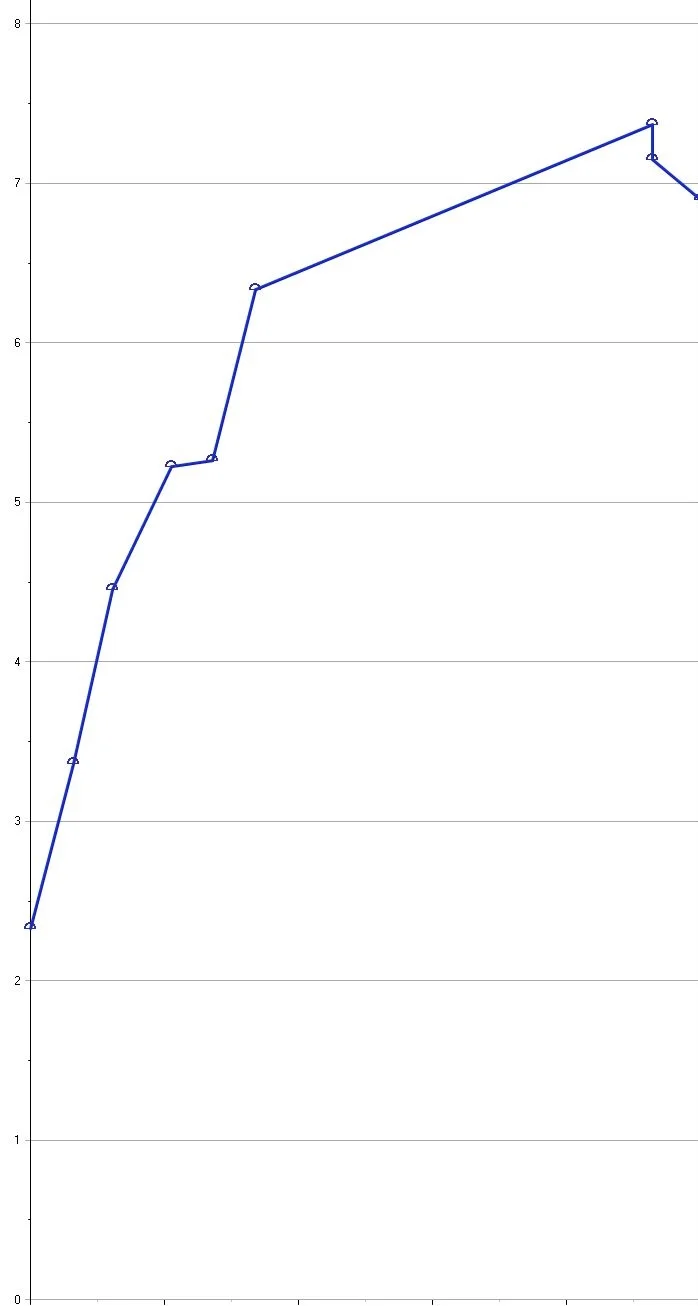
Troponin trend: Obviously positive! The negative echo and cath make the case interesting.

MRI: Small focus of transmural delayed enhancement in the inferior wall (missing piece of the donut), consistent with a myocardial infarction.

Conventional CT, short axis plane: Underwhelming.

Iodine map, short axis plane: The perfusion defect is obvious!

Perfusion defect shown very nicely on iodine overlay. Note how well it corresponds to the delayed enhancement on MRI.